









Near the heart of the spreading Ebola outbreak, young mother Marléne is well aware of the potential danger.
She’s brought her two-month-old daughter, Deborah, to be vaccinated at a health facility in the eastern Democratic Republic of Congo.
The north-eastern region of Ituri has so far seen more than 100 confirmed cases of the disease, with more in neighbouring North Kivu.
Marléne, whose name has been changed due to the stigma surrounding Ebola, sees the damage the disease can do through images shared online.
“From what we see circulating on phones, we notice the symptoms,” she says, speaking to health workers from nonprofit Save the Children.
“People say the disease is transmitted through contact. For example, if I am infected, through sweat my child could also become infected.
“This is what worries us the most — how we can protect our children.”
Tensions are running high — according to the World Health Organization, violence against health facilities and community resistance is proving a major barrier to combating the outbreak.
But this is the 17th Ebola outbreak the DRC has faced since 1976. It is not unprepared.



Perth GP Dr Saschveen Singh has been working with Médecins Sans Frontières (MSF) since 2017, and was on the ground during the last major Ebola virus outbreak in the DRC in 2018-19.
For now, she’s based out of the organisation’s Paris headquarters, a member of the epidemic response team supporting their emergency response.
Two of her colleagues have already flown out to the front line, and Dr Singh is on call to do the same in coming weeks.

The big problem, she says, is while the outbreak rages on, the “routine” work continues.
“We have to ensure … pregnant women can access important antenatal support, and that they can deliver safely,” she says.
“[There are] children and adults with malaria. That is a really rapidly fatal disease … we need to ensure they are diagnosed and treated rapidly so they don’t end up in hospital.
“There’s still people with tuberculosis, with HIV, with diabetes, they need to be able to access their ongoing drugs.
“We don’t want the whole system collapsing because all the effort is on a particular infectious disease response.“
Race against time to determine the true number of cases
Efforts to contain the ongoing outbreak are unfolding in what the United Nations called “one of the most volatile” regions of the eastern DRC.
As of May 29, there have been 906 suspected cases, and 223 suspected deaths.
The word “suspected” is key.
Unlike other Ebola virus outbreaks, this time transmission comes from a rarer form of the disease, known as Bundibugyo virus.
It’s spread through bodily fluids, has similar early symptoms to the common cold, and there is no currently approved vaccine.
Health officials on the ground are dealing with a shortage of Bundibugyo-specific virus testing kits while battling a number of other diseases also common in the area.

The lack of confirmation, according to Dr Singh, means the true scale of the outbreak is difficult to determine.
Of the more than 1,100 suspected cases sampled, she says, less than 10 per cent had been confirmed.
“And what that indicates to us is that there’s a critical gap in diagnosis, there’s a whole number of patients … being isolated as suspected cases,” she says.
“But there’s such a big delay in actually being able to either confirm or refute their diagnosis, that really slows down the epidemiological response and contact tracing.
“We really, really need to urgently scale up testing capacity.“
The number of suspected and confirmed cases is rising rapidly, and the number of people on the list for contact tracing has surpassed 2,630.
In the span of eight days, the number of suspected cases increased by 160.
In the WHO’s May 29 situation report, they record 134 confirmed cases, nine of which are in Uganda, and 18 confirmed deaths.
Among those confirmed deaths were three Red Cross volunteers, who likely caught the disease while managing dead bodies on March 27.
Alikana Udumusi Augustin, Sezabo Katanabo, and Ajiko Chandiru Viviane were working on a “humanitarian mission unrelated to Ebola”, according to their organisation.
They would have been exposed before the outbreak had been identified, and are among the first known victims of the outbreak.
Also exposed was an American doctor, who tested positive on May 17 and has since been transported to Germany for treatment.
‘Imagine taking the entire population of the Gold Coast and dropping it into … Sydney’
Another factor complicating things for those on the ground is what the WHO is calling a “catastrophic collision of disease and conflict”.
The DRC is the site of one of the most complex displacement crises on the planet, according to the United Nations High Commissioner for Refugees (UNHCR).
Conflict, instability, epidemics and climate shock have taken a severe toll on the country.
A decades-long struggle for independence now sees militant and rebel groups, the Congolese armed forces and foreign forces battling for control.
Rachel Criswell, the UNHCR spokesperson in the Congo, says there are almost 1 million displaced people at the epicentre of the situation.



That conflict affects every aspect of getting the Ebola outbreak under control.
“Imagine taking the entire population of the Gold Coast and dropping it into the middle of Sydney,” Ms Criswell says.
“That’s what we’ve been having happen in this period of time.
“In the month of April alone, 26,000 people [were] dropped in neighbouring communities because of conflict.“
Those displaced people are living with friends, in humanitarian tented communities, or in schools and churches.
Those contexts, Ms Criswell notes, make things like handwashing and isolating at the first sign of sickness difficult.
“And remember, the initial symptoms of Ebola are the same as the common flu,” she says.
“There will be a lot of people who need to separate themselves to see if they have continuing symptoms or if it’s just a regular flu.”

By the time lab testing confirmed the outbreak of Bundibugyo virus, the disease had already spread.
The available Ebola testing kits, designed to pick up the more common Zaire virus, were all coming back negative.
Greg Ramm, Save the Children’s country director in the DRC, says that delay has left humanitarian groups behind the curve.


They already know what to do to fight an Ebola outbreak.
“[But] the problem now isn’t that it’s a different strain, it’s that it’s spread already to 10 health zones across Ituri province and North Kivu province,” he says.
“That means getting on top of it is going to be very hard.“
Congo ‘not starting from square one’ as vaccine develops
Groups like Save the Children say they’re launching large-scale responses in an area where health systems are already fragile.
Supporting their staff and keeping their programs and health centres up and running, says Mr Ramm, is their “first and most urgent priority”.
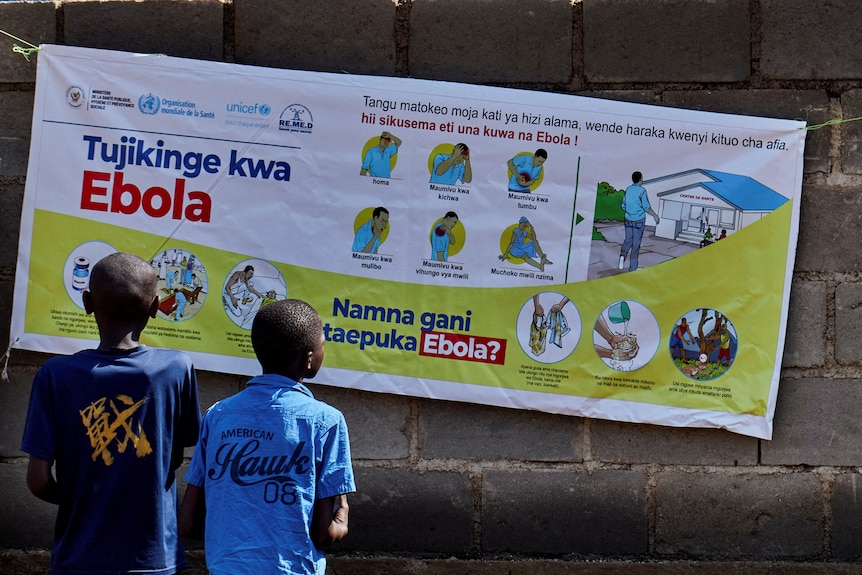
“In addition, we are working very hard to get out messages across the community,” he says.
“This is the biggest outbreak Ituri province has ever known.“
“We demystify [Ebola], fight the rumours, make sure communities understand what they need to do to keep themselves safe, keep their families safe, keep their community safe.”
After the outbreak, Save the Children scaled up its support to health facilities, providing comprehensive infection prevention and increasing hygiene measures.

MSF has begun constructing a 65-bed Ebola treatment centre to admit both confirmed and suspected cases.
In Ituri’s capital, an isolation system has been set up for patients in its largest hospital.
The UNHCR last week worked with 10,000 South Sudanese refugees in Ituri, educating them on the key steps stopping the spread of the disease.
Rapid work is also underway to develop a vaccine.
The WHO said last week its expert had determined the “most promising candidate vaccine” was a single-dose shot using the same platform as the only licensed Ebola vaccine.
They estimated it would take seven to nine months for it to be ready for human testing.
For Ms Criswell, the closest comparison is the difference between a “bad bushfire year and a sensible bushfire year”.
“Here in Congo, we don’t have problems with bushfires … but epidemics like Ebola, like Mpox, are a regular situation,” she says.
“Our last outbreak actually just ended in December of 2025.
“But … normally we’re able to rely on the stocks of vaccines to quickly treat the first contact cases. We can’t do that right now.”


The lack of a vaccine and the outbreak hitting urban and semi-urban areas, along with the ongoing conflict, means this is a bad year.
“We’re not starting from square one,” she says.
“Ebola has been present in Congo my entire life and the life of almost all my colleagues.
“Just like [what] you would all know to do with bushfires … they have the ability, the reflexes to deal with that here.
“And you have some of the world’s top experts on this epidemic form Congo working on this situation right now.”



